
76 years old man was brought to A&E with h/o alleged assault. He was punched and kicked on his chest by his daughter. He was complaining to central chest pain. There was no h/o palpitation, SOB or collapse. He was known to have IHD and had undergone cardiac bypass surgery 4 weeks ago.
Examination findings are as follows:
PR- 68/min
BP- 130/ 68
Heart sounds- Normal. No pericardial rub/ murmur
Lungs: Bilateral equal air entry. No adventitious sounds
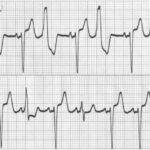
ECG: Sinus rhythm @84/min with frequent ventricular ectopics
How to diagnose cardiac injury in blunt chest wall trauma?
My Learning:
Blunt cardiac injury (BCI) refers to injury sustained due to blunt trauma to the heart which is more common than penetrating injuries.[1]
The incidence of cardiac injury following blunt chest trauma varies between 8% and 86%.[2]
Most common mechanism is high-speed vehicle collision. This is followed by falls from height or crushing incidents.[3]
Cardiac manifestations include arrhythmias, wall motion abnormalities, myocardial wall rupture, and valve damage. However, the most prevalent pathology is myocardial contusion.
Clinical features:
Commotio cordis:
Commotio cordis is defined as sudden cardiac death triggered by a relatively innocent blow to the precordium over the left chest wall.[4] Collapse typically follows instantaneously or within a few seconds due to arrhythmias (typically ventricular fibrillation [VF]).
Coronary artery dissection:
Almost 2% of coronary artery injuries can be related to BCI, causing coronary artery dissection that leads to myocardial ischemia.[9,10] The most commonly involved artery is the left anterior descending artery [5].
Pericardial effusion and tamponade:
With traumatic cardiac injuries, effusions are more commonly haemorrhagic, either due to damage to the integrity of the myocardial wall or its vessels causing bleeding into the pericardial sac, or due to traumatic pericarditis. Many case reports indicated right wall rupture as the source of leakage[6]
Traumatic cardiac arrest:
TCA is a consequence of hypovolemia due to blood loss characterized by a very low cardiac output state.
Although other viable options of management such as chest compressions and adrenaline are available for medical cardiac arrest, no positive outcome has been recorded for TCA with these options.[20]
Blunt aortic injury:
Traumatic rupture of the thoracic aorta is a life-threatening condition, and it is the second most common cause of death after head injury. 90% of patients die at the scene. Blunt aortic injury (BAI) occurs with rapid deceleration in road traffic accidents or falls [8]
DIAGNOSIS
Electrocardiography
Electrocardiography has consistently proven to be the best predictor of blunt cardiac trauma [19] but is insufficient to completely exclude the diagnosis based only on ECG.
Common ECG manifestations include ventricular ectopics, atrial fibrillation or flutter, new conduction blocks and ST- T changes.
Chest X-ray
X-ray findings are not a definite tool for cardiac diagnosis, but it may reveal significant findings such as fractures, air collection, hematomas, or heart enlargement.
Focused assessment with sonography for trauma
FAST is a preliminary investigative tool to view not only the heart but also the chest and abdominal cavities in a setting of trauma diagnosis and management.[11]
Echocardiography
In expert hands echocardiography provides the opportunity to visualize the heart with all its chambers, valves, pressure, ejection fraction, wall abnormalities, and pericardium. Early assessment with echo leads to accurate diagnosis in case of anterior chest wall injury and management of pericardial effusion.[12]
Coronary computed tomography angiography
It is a superior method of viewing the coronary arteries noninvasively. It provides a better description to highlight partial myocardial rupture and ventricular septal defect in relation to the coronary vessels.[13]
BOTTOM LINE
Patients with blunt thoracic trauma should be investigated with cardiac biomarkers (e.g., Troponin) in the presence of abnormal ECG or haemodynamic instability. If it is elevated, cardiac biomarkers should be repeated after 3 hours
Haemodynamically stable patients with normal ECG and normal cardiac biomarkers at presentation are unlikely to have sustained significant cardiac injury.
References:
- El-Menyar A, Al Thani H, Zarour A, Latifi R. Understanding traumatic blunt cardiac injury. Ann Card Anaesth. 2012;15:287–95
- Akar İ, İnce İ, Aslan C, Çeber M, Kaya İ. Left atrial rupture due to blunt thoracic trauma. Ulus Travma Acil Cerrahi Derg. 2015;21:303–5
- Link MS. Commotio the: Ventricular fibrillation triggered by chest impact-induced abnormalities in repolarization. Circ Arrhythm Electrophysiol. 2012;5:425–32
- 5. Walker J, Calkins H, Nazarian S. Evaluation of cardiac arrhythmia among athletes. Am J Med. 2010;123:1075–81.
- Lin YL, Yu CH. A cute myocardial infarction caused by coronary artery dissection after a blunt chest trauma. Intern Med. 2011;50:1969–71.
- Sadr-Ameli MA, Amiri E, Pouraliakbar H, Heidarali M. Left anterior descending coronary artery dissection after blunt chest trauma. Arch Iran Med. 2014;17:86–90
- Evans CC, Petersen A, Meier EN, Buick JE, Schreiber M, Kannas D, et al. Prehospital traumatic cardiac arrest: Management and outcomes from the resuscitation outcomes consortium epistry-trauma and PROPHET registries. J Trauma Acute Care Surg. 2016;81:285–93
- Di Marco L, Pacini D, Di Bartolomeo R. A cute traumatic thoracic aortic injury: Considerations and reflections on the endovascular aneurysm repair. Aorta (Stamford) 2013;1:117–22.
- Audette JS, Emond M, Scott H, Lortie G. Investigation of myocardial contusion with sternal fracture in the emergency department: Multicentre review. Can Fam Physician. 2014;60:e126–30.
- Ghalem A, Boussir H, Ahsayan K, Ismaili N, Ouafi NE. ST-segment elevation after blunt chest trauma: Myocardial contusion with normal coronary arteries or myocardial infarction following coronary lesions. Pan Afr Med J. 2017;28:26.
- Baker L, Almadani A, Ball CG. False negative pericardial focused assessment with sonography for trauma examination following cardiac rupture from blunt thoracic trauma: A case report. J Med Case Rep. 2015;9:155
- Karaca O, Demir G, Özyüksel A, Akçevin A. Tricuspid valve chordal rupture after a motorbike accident. Turk Kardiyol Dern Ars. 2016;44:329–31.
- Rojas CA, Cruite DM, Chung JH. Traumatic ventricular septal defect: Characterization with electrocardiogram-gated cardiac computed tomography angiography. J Thorac Imaging. 2012;27:W174–6
- Mishra B, Gupta A, Sagar S, Singhal M, Kumar S. Traumatic cardiac injury: Experience from a level-1 trauma centre. Chin J Traumatol. 2016;19:333–6.
- Slessor D, Hunter S. To be blunt: Are we wasting our time. Emergency department thoracotomy following blunt trauma: A systematic review and meta-analysis? Ann Emerg Med. 2015;65:297–307.e16.
- Rabin J, DuBose J, Sliker CW, O’Connor JV, Scalea TM, Griffith BP. Parameters for successful nonoperative management of traumatic aortic injury. J Thorac Cardiovasc Surg. 2014;147:143–9
17 . Di Marco L, Pacini D, Di Bartolomeo R. A cute traumatic thoracic aortic injury: Considerations and reflections on the endovascular aneurysm repair. Aorta (Stamford) 2013;1:117–22
- Clancy K, Velopulos C, Bilaniuk JW, Collier B, Crowley W, Kurek S, et al. Screening for blunt cardiac injury: An eastern association for the surgery of trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S301–6.
- Fulda GJ, Giberson F, Hailstone D, Law A, Stillabower M. An evaluation of serum troponin T and signal-averaged electrocardiography in predicting electrocardiographic abnormalities after blunt chest trauma. J Trauma. 1997;43(2):304–10
- Velmahos GC, Karaiskakis M, Salim A, Toutouzas KG, Murray J, Asensio J, et al. Normal electrocardiography and serum troponin I levels preclude the presence of clinically significant blunt cardiac injury. J Trauma. 2003;54(1):45–50
- Yousef R, Carr JA. Blunt cardiac trauma: a review of the current knowledge and management. Ann Thorac Surg. 2014;98(3):1134–1140. doi: 10.1016/j.athoracsur.2014.04.043.
- Van Lieshout EMM, Verhofstad MHJ, Van Silfhout DJT, Dubois EA. Diagnostic approach for myocardial contusion: a retrospective evaluation of patient data and review of the literature. Eur J Trauma Emerg Surg. 2021;47(4):1259-1272.