
84 years old man brought to A&E by ambulance with h/o chest pain. He was pre alerted as NSTEMI with ST depression in anterior chest leads. He gave h/o central chest pain for past 4 hours. It was like tightness/heaviness in nature with pain score of 9/10 despite Aspirin, GTN and Morphine by paramedics prior to arrival in A&E.
His past medical history included hypertension for which he was taking medications. He was otherwise in good health and denied any other medical problems.
His examination findings and vitals are as follows:
Temp. 36.9 C
PR- 64/ min, regular
BP- 162/ 72 mm Hg
O2 saturation- 98% on room air
Heart and lungs examination was normal.
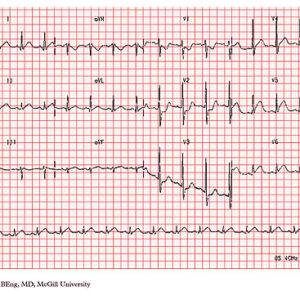
ECG:
normal sinus rhythm @ 78/ min, ST depression (about 2-3mm) in V2-V3 with positive T waves. No other ST-T changes noted in other leads. (ECG shown above does not belong to this patient)
Diagnosis of acute posterior wall MI was suspected in view of history and ECG changes.
He was referred to cardiologist who agreed with the diagnosis and the need for primary PCI. As he was waiting for transfer to Cath lab and the cardiologist by bedside, he developed ventricular tachycardia @200/min. His BP was 150/minute.
He was commenced on Amiodarone bolus on advice of Cardiologist and transferred to Cath lab. He was subsequently cardioverted later. He was found to have occlusion of circumflex artery which was treated with 1 stent. He made full recovery and was discharged home after few days.
My learning:
ECG criteria for diagnosis of posterior wall MI
On a standard 12-lead ECG Posterior MI is suggested by following ECG changes in precordial leads (V1- V4) [1,2]
- ST-segment depression in precordial leads
- Prominent R wave
- R/S wave ratio >1.0 in lead V2
- Prominent, upright T waves
In addition, there may be
- Co-existing acute inferior and/or lateral MI
- Additional lead ECG (posterior leads V7 to V9) may reveal ≥ 1 mm ST-segment elevation
Discussion:
Precordial ST-depression may be attributable to either posterior wall MI or subendocardial ischemia (NSTEMI). Evidence suggests that the ST depression of posterior MI is maximal in V1-V4, whereas the ST depression of subendocardial ischemia is maximal in V5 and V6.
I have found following YouTube video (bottom of this page) very informative.
References:
1.Electrocardiographic evolution of posterior acute myocardial infarction: importance of early precordial ST-segment depression.
Boden WE, Kleiger RE, Gibson RS, Schwartz DJ, Schechtman KB, Capone RJ, Roberts R.
Am J Cardiol. 1987 Apr 1;59(8):782-7. doi: 10.1016/0002-9149(87)91091-5. PMID: 3825938.
2.Posterior myocardial infarction: the dark side of the moon.
van Gorselen EO, Verheugt FW, Meursing BT, Oude Ophuis AJ.
Neth Heart J. 2007;15(1):16-21.