
73 years old woman was brought to A&E with h/o palpitations. She gave h/o on and off episodes of palpitations for one week. There was no h/o chest pain/ SOB or collapse. Her past medical history included hypertension and hypercholesterolaemia.
Examination findings are as follows:
Temp. 36.9 C
PR- 152/min (on monitor)
BP- 116/70 mm Hg
Heart/ chest examination- normal
O2 saturation- 96% on room air
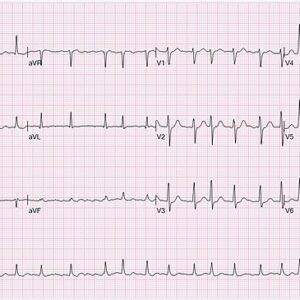
ECG- AF @155/min, no significant ST-T changes
CXR- nil significant
Background:
As per NICE guidelines on management of atrial fibrillation ( last updated: 30 June 2021) beta blockers are the first choice for rate control [1]. It does not give any preference to Bisoprolol over Metoprolol. I have also reviewed European and American guidelines which give similar advice.
In our trust, Bisoprolol appears to be the drug of choice in this situation and preferred by cardiologist over metoprolol (as per my observation). I did not find any randomised controlled trials comparing these two medications. I decided to learn somewhat in depth about pharmacology of beta blockers.
My learning:
Beta-blockers are classified according to their adrenoceptor binding affinities.
There are three main sub-types of beta-adrenoceptors:
Beta1-adrenoceptors (75%) are located in the heart. Activation of the beta-1 receptor in the heart increases heart rate and contractility [2]
Beta2-adrenoceptors are located in vascular and bronchial smooth muscle, Activation lead to smooth muscle relaxation and bronchodilation
Beta3-adrenoceptors are located on adipocytes and are thought to be involved with fatty acid metabolism
Properties of beta-blockers
Beta-blocker Selectivity
Atenolol β1 selective
Bisoprolol β1 selective++
Metoprolol β1 selective+
Propranolol Non-selective
Sotalol Non-selective
Cardio selective beta-blockers, e.g. atenolol, bisoprolol and metoprolol, have a greater affinity for beta1-adrenoceptors and are less likely to cause constriction of airways or peripheral vasculature and are preferred in patients with respiratory disease. Bisoprolol is reported to be more cardio selective than metoprolol and atenolol [3].
Non-selective beta-blockers, e.g. propranolol, block beta1 and beta2-adrenoceptors equally.
Pharmacokinetics:
Metoprolol
Onset: 20 min (IV), when infused over 10 min; onset may be immediate, depending on clinical setting; 1-2 hr (PO)
Duration: 3-6 hr (PO); duration is dose-related; 24 hr (Prolonged release);
5-8 hr (IV)
Peak plasma time: 1.5-2 hr (immediate-release); 3.3 hr (extended-release)
Bisoprolol
Onset of Action: 1 to 2 hours
Time to Peak: 2 to 4 hours
Half-Life Elimination: 9 to 12 hours (normal renal function) ; CrCl <40 mL/minute: 27 to 36 hours; Hepatic cirrhosis: 8 to 22 hours
Take home message:
Choice between Metoprolol vs Bisoprolol depends on the urgency of clinical situation. If rapid control of ventricular rate is required Metoprolol 5mg IV over 2 minute can be administered. In other situations Bisoprolol appears to be preferred choice as it is more cardio selective compared to metoprolol.
References:
1.https://www.nice.org.uk/guidance/ng196
2.Alhayek S, Preuss CV. Beta 1 Receptors. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL):StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532904/
3.Michael A. Weber, The Role of the New β-Blockers in Treating Cardiovascular Disease, American Journal of Hypertension, Volume 18, Issue S6, December 2005, Pages 169S–176S
4.https://reference.medscape.com/drugs/beta-blockers-beta-1-selective
5.https://www.medicine.com/drug/bisoprolol/hcp